What Exactly Is Peripheral Artery Disease?
Peripheral Artery Disease (PAD) — sometimes called peripheral vascular disease (PVD) or peripheral arterial occlusive disease (PAOD) — is a common circulatory condition in which narrowed arteries reduce blood flow to the limbs. In the vast majority of cases, PAD affects the arteries that supply the legs and feet.
"Peripheral" simply means outside the heart and brain. While coronary artery disease affects the arteries feeding the heart, and carotid artery disease affects the arteries feeding the brain, PAD affects the arteries feeding the extremities — most commonly the legs.
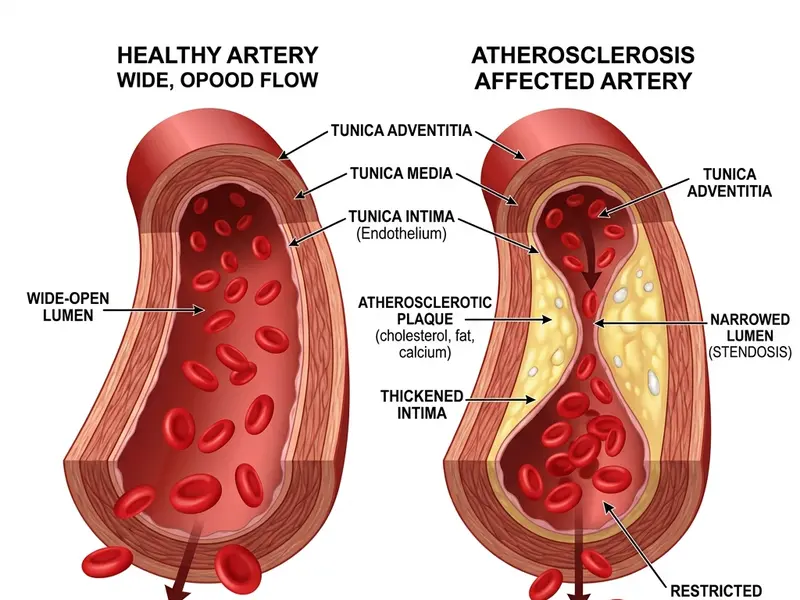
The fundamental mechanism is the same across all three: atherosclerosis — the progressive buildup of fatty plaques inside artery walls that narrows the channel and restricts blood flow. This makes PAD, coronary artery disease, and carotid artery disease manifestations of the same underlying systemic disease process, just in different locations.
Up to 50% of people with PAD have no symptoms whatsoever. They walk through life unaware that their leg arteries are progressively narrowing and their cardiovascular risk is climbing. This is why ABI screening for high-risk individuals is so important — it catches PAD before it becomes dangerous.
How Common Is PAD in the USA and Canada?
PAD is far more prevalent than most people realize, and it's growing:
PAD prevalence increases dramatically with age. Based on data from the American College of Cardiology:
- Approximately 2–3% of people aged 40–49 have PAD
- 7–10% of those aged 60–69
- 15–20% of those over 70
- Among Black Americans over 80, some studies have found PAD prevalence exceeding 50% — a stark disparity linked to higher rates of diabetes, hypertension, and limited healthcare access
In Canada, the Canadian Cardiovascular Society notes that PAD is significantly underdiagnosed, particularly in women and in communities with lower healthcare access. Indigenous communities in Canada face disproportionately high rates of diabetes-related PAD.
What Causes PAD?
The overwhelming majority of PAD cases are caused by atherosclerosis. Certain factors dramatically increase the likelihood of developing it:
Major Risk Factors
- Smoking: This is the #1 modifiable risk factor for PAD. Smokers are 2–4 times more likely to develop PAD than non-smokers. The chemicals in cigarette smoke directly damage artery walls, accelerate plaque formation, and cause vasoconstriction (artery narrowing). Former smokers retain elevated risk for years after quitting.
- Diabetes: Diabetic patients develop PAD earlier, more severely, and more diffusely than non-diabetics. High blood glucose damages the artery walls and promotes inflammation and plaque formation. Diabetics with PAD are also more likely to have the calcified arteries that make ABI unreliable — requiring a TBI test instead. Read more about PAD and diabetes →
- High blood pressure (Hypertension): Sustained high pressure against artery walls causes microscopic damage that accelerates atherosclerosis.
- High cholesterol (Dyslipidemia): Elevated LDL ("bad cholesterol") and triglycerides promote plaque buildup. Low HDL ("good cholesterol") is also associated with higher PAD risk.
- Age: The risk of PAD increases substantially after age 50 and rises sharply after 65. Arteries naturally become stiffer and less elastic with age, making them more vulnerable to disease.
- Family history: First-degree relatives of PAD patients have 2–3 times higher risk of developing the condition themselves.
Less Common Causes
While atherosclerosis accounts for over 90% of PAD cases, other causes include:
- Inflammatory conditions: Vasculitis (inflammation of blood vessels), including Buerger's disease (thromboangiitis obliterans) — strongly associated with tobacco use
- Blood clotting disorders: Conditions that increase clot formation can cause acute arterial occlusion
- Popliteal artery entrapment syndrome: A rare condition in young athletes where the popliteal artery behind the knee is compressed by abnormal muscle or fibrous tissue
- Fibromuscular dysplasia: A non-inflammatory arterial disease affecting younger women, most commonly affecting renal and carotid arteries but occasionally leg arteries
How Atherosclerosis Damages Arteries Over Time
Understanding atherosclerosis helps make sense of why PAD develops gradually over decades — and why early intervention matters so much:
Phase 1 — Endothelial Damage (often begins in the 20s–30s): The inner lining of arteries (the endothelium) is damaged by risk factors: cigarette toxins, high blood pressure, excess glucose. This damage is microscopic and produces no symptoms.
Phase 2 — Plaque Formation: LDL cholesterol particles penetrate the damaged endothelium and become oxidized. The immune system recognizes these as a threat and sends white blood cells (macrophages) to consume them. These macrophages become "foam cells" that accumulate in the artery wall, creating a fatty streak — the earliest visible form of atherosclerosis.
Phase 3 — Plaque Growth: Over years and decades, the fatty streaks grow into mature plaques (atheromas) that bulge into the artery's interior, progressively narrowing the channel. A fibrous cap forms over the plaque. The artery begins to stiffen and lose elasticity.
Phase 4 — Plaque Rupture or Critical Narrowing: When a plaque ruptures, blood clots form rapidly at the rupture site. In coronary arteries, this causes a heart attack. In leg arteries, this can cause sudden severe ischemia ("acute limb ischemia"), which is a surgical emergency. Alternatively, a plaque that grows slowly enough can narrow the artery to 70% or more of its diameter before causing symptoms (like claudication).
The Stages of PAD — Fontaine Classification
The Fontaine Classification, developed by French surgeon René Fontaine in 1954, remains one of the most widely used systems for staging PAD severity:
| Stage | Clinical Features | Typical ABI Range |
|---|---|---|
| Stage I | Asymptomatic — PAD present but no symptoms | 0.8–0.9 or lower |
| Stage IIa | Mild claudication — pain occurs after walking >200m | 0.7–0.9 |
| Stage IIb | Moderate/severe claudication — pain after <200m | 0.5–0.7 |
| Stage III | Ischemic rest pain — pain at rest, especially at night | 0.4–0.6 |
| Stage IV | Ischemic ulcers or gangrene — tissue death | Often <0.4 |
Stages III and IV together are called Critical Limb-Threatening Ischemia (CLTI) — a medical urgency requiring prompt vascular specialist care.
PAD Is Not Just a Leg Problem — The Systemic Risk
This is perhaps the most important thing PAD patients need to understand: PAD is a marker of systemic cardiovascular disease. The same atherosclerotic process that has blocked arteries in your legs has almost certainly affected arteries elsewhere in your body.
Research consistently shows that people with PAD have dramatically elevated rates of heart attack, stroke, and cardiovascular death:
- PAD patients have a 2–4 times higher risk of major cardiovascular events over 10 years compared to people without PAD
- Up to 60% of people with PAD also have coronary artery disease (narrowed heart arteries)
- Up to 30–40% have carotid artery disease (narrowed neck arteries supplying the brain)
- The 5-year mortality rate for people with symptomatic PAD is approximately 30% — predominantly from heart attack and stroke, not from leg complications
This is why PAD is not treated in isolation. When a vascular specialist diagnoses PAD, they are simultaneously managing the patient's entire cardiovascular risk profile — not just the leg symptoms.
How Is PAD Diagnosed?
The diagnostic pathway for PAD typically begins with a clinical history and physical examination, followed by non-invasive testing:
- ABI Test: The first-line, most accessible test. An ABI below 0.9 is diagnostic for PAD. Learn how the test is performed →
- Toe-Brachial Index (TBI): Used when ABI is unreliable (ABI >1.4 in diabetics). Compare ABI and TBI →
- Duplex Ultrasound: Combines B-mode ultrasound (seeing the artery anatomy) with Doppler (measuring flow velocity) to locate the precise site and severity of stenosis or occlusion
- CT Angiography (CTA): A CT scan using intravenous contrast that produces detailed 3D images of the arteries. Used to plan endovascular or surgical procedures
- MR Angiography (MRA): Similar to CTA but without radiation. Used in patients who can't receive contrast dye (kidney disease)
- Conventional Catheter Angiography: The gold standard for arterial imaging — a catheter is inserted (usually through the groin) and contrast dye injected directly into the arteries. Now used primarily just before endovascular treatment
What Happens If PAD Goes Untreated?
PAD is a progressive disease. Without intervention — whether lifestyle, medical, or procedural — most cases worsen over time. The natural history data paints a concerning picture:
- About 25% of claudication patients will progress to more severe symptoms within 5 years
- 5–10% will progress to critical limb ischemia within 5 years, with a significant risk of amputation
- The cardiovascular mortality risk is cumulative — each year of untreated PAD represents another year of elevated heart attack and stroke risk
The encouraging news is that with appropriate treatment — a combination of risk factor modification, medical therapy, and when needed, revascularization — most patients with PAD can maintain good quality of life, preserve their limbs, and meaningfully reduce their cardiovascular risk. Explore all PAD treatment options →