- What Is Intermittent Claudication?
- The Physiology: Why It Hurts
- Where Claudication Pain Is Felt (and What It Means)
- Grading Claudication: Fontaine & Rutherford Systems
- How Is Claudication Diagnosed?
- Conditions That Mimic Claudication
- Natural History: Will It Get Worse?
- Treatment for Claudication
- FAQs
What Is Intermittent Claudication?
The term "claudication" comes from the Latin claudicare, meaning to limp. "Intermittent" describes its defining characteristic: it comes and goes. Specifically, intermittent claudication is muscle pain, cramping, heaviness, or fatigue in the legs that:
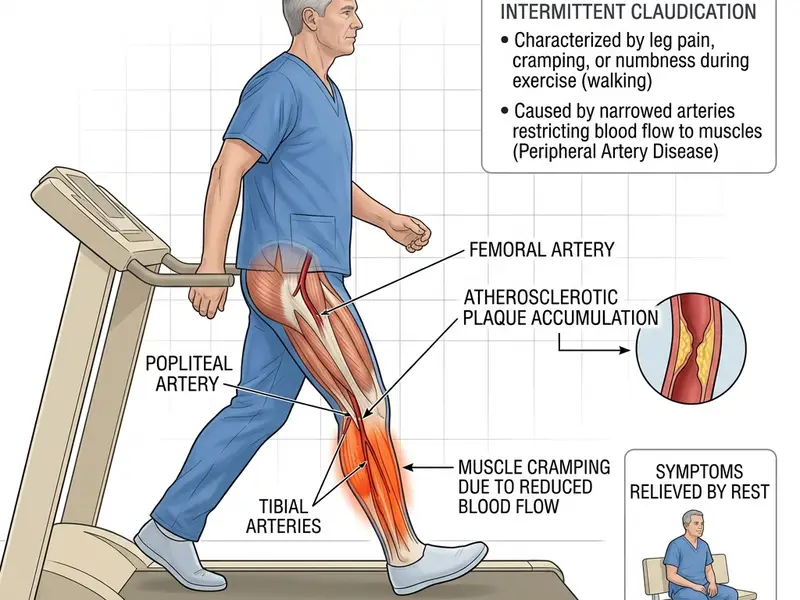
- Starts during walking or physical exertion
- Occurs predictably after a consistent walking distance
- Completely resolves within 1–5 minutes of stopping (standing still — not necessarily sitting down)
- Returns at the same distance when walking resumes
This precise pattern — exertion on, rest off — is the clinical hallmark of arterial insufficiency. It distinguishes claudication from other causes of leg pain (arthritis, nerve pain, venous disease) with remarkable specificity. Vascular surgeons often diagnose claudication from the history alone before any testing is done.
Claudication is the most common symptomatic presentation of Peripheral Artery Disease (PAD). It affects approximately 3–5% of people over 50 in the USA and Canada, though the true prevalence is probably higher due to underreporting and misattribution of symptoms.
The Physiology: Why It Hurts
Understanding why claudication happens requires understanding how arteries and muscles interact during exercise.
At Rest
Even with significant arterial narrowing, resting blood flow to the leg muscles is often adequate. Muscles at rest have relatively low oxygen demands, and the blood flow through the narrowed artery — while reduced — may be sufficient. This is why many PAD patients feel completely normal when sedentary.
During Exercise
When you start walking, your leg muscles suddenly need dramatically more oxygen — the demand can increase 5–10 fold. In a healthy leg, the arteries dilate to deliver this increased supply. In a PAD-affected leg, the narrowed artery cannot dilate properly, and blood flow increase is limited by the stenosis (blockage).
When oxygen delivery falls below demand, the muscle cells switch to anaerobic metabolism — they make energy without oxygen. This process produces lactic acid and other metabolic byproducts that accumulate in the muscle tissue. These chemicals activate pain receptors (nociceptors) in the muscle, producing the characteristic burning, cramping sensation of claudication.
At Rest Again
When you stop walking, muscle oxygen demand drops immediately back to resting levels. The blood flow, limited though it is, quickly re-establishes adequate oxygen supply. Lactic acid and other metabolic waste products are cleared within 1–5 minutes, and pain resolves completely. This rapid, complete resolution is key — if pain persists for more than 10–15 minutes at rest, it suggests more severe disease than simple claudication.
Where Claudication Is Felt — and What It Tells You
The location of claudication pain is a powerful clue about where the arterial blockage is located:
| Pain Location | Most Likely Blocked Artery | Notes |
|---|---|---|
| Calf (most common — 80% of cases) | Superficial femoral artery or popliteal artery | The classic location — cramping in the back of the lower leg |
| Thigh | Femoral artery (mid-thigh) | Less common; often combined with calf claudication |
| Buttock and hip | Iliac artery (pelvis) | May also cause erectile dysfunction in men (Leriche syndrome) |
| Foot | Tibial arteries (below knee) | Less common; particularly in diabetics with distal PAD |
| Bilateral buttock + thigh + calf | Aortoiliac disease | Leriche syndrome — also includes impotence in men; requires major surgery or aortobifemoral bypass |
Grading Claudication Severity
Two clinical grading systems are used for PAD and claudication:
Fontaine Classification
The older, simpler system — widely used in Europe and Canada:
- Stage I: Asymptomatic PAD (no claudication)
- Stage IIa: Claudication occurring after more than 200 meters of walking (mild)
- Stage IIb: Claudication occurring after less than 200 meters (moderate to severe)
- Stage III: Ischemic rest pain
- Stage IV: Tissue loss (ulcers or gangrene)
Rutherford Classification
The more nuanced system used in contemporary vascular research and American clinical practice:
| Rutherford Category | Description |
|---|---|
| Category 0 | Asymptomatic — ABI abnormal but no symptoms |
| Category 1 | Mild claudication |
| Category 2 | Moderate claudication |
| Category 3 | Severe claudication (less than 200m pain-free distance) |
| Category 4 | Ischemic rest pain |
| Category 5 | Minor tissue loss (ulcer not full thickness) |
| Category 6 | Major tissue loss / gangrene |
Categories 1–3 are claudication; categories 4–6 represent Critical Limb-Threatening Ischemia (CLTI).
How Is Claudication Diagnosed?
Claudication is primarily a clinical diagnosis — made from the history. The physician will then confirm it with objective testing:
- Physical examination: Diminished or absent pedal pulses (dorsalis pedis and posterior tibial), arterial bruits over the femoral artery, and skin changes (hair loss, shiny skin, color changes)
- ABI test: The first-line objective test. ABI below 0.9 confirms PAD. ABI typically 0.5–0.9 in claudication. Calculate your ABI →
- Exercise ABI: If resting ABI is normal but symptoms are classic, an exercise ABI (treadmill test) is performed — a significant drop in ABI after exercise is diagnostic
- Duplex ultrasound: Identifies the location and severity of arterial lesions if intervention is being planned
Conditions That Mimic Claudication (Differential Diagnosis)
Not all leg pain with walking is arterial claudication. Key mimics:
- Neurogenic claudication (lumbar spinal stenosis): Back or buttock pain radiating to the legs during walking. Distinguished by: also occurs with prolonged standing; relieved by sitting (specifically spinal flexion); pain pattern often more diffuse; bicycle exercise typically well-tolerated (unlike arterial claudication); normal ABI.
- Venous claudication: Tight, bursting, "exploding" sensation during walking; associated with leg swelling; improved by leg elevation (opposite of arterial disease). Occurs in patients with severe venous obstruction (e.g., post-DVT syndrome).
- Chronic compartment syndrome: Pain specifically in the anterior shin compartment during running; common in young athletes; exercise-induced pressure buildup in a fascial compartment; normal ABI.
- Hip osteoarthritis: Groin pain with activity that may radiate to the thigh; worsens with specific hip movements; doesn't follow predictable walking distance pattern; X-ray shows joint changes.
- Popliteal artery entrapment syndrome: Young athletes with calf pain during running; caused by abnormal muscle or fibrous band compressing the popliteal artery; ABI may be normal at rest but drops dramatically during plantar flexion maneuver.
Natural History: What Happens If You Don't Treat Claudication?
The natural history of claudication is important context for treatment decisions:
- Over 5 years, approximately 70–75% of claudication patients remain stable or improve — their claudication stays the same or gets better, particularly if they exercise and address risk factors
- Approximately 10–15% will experience worsening claudication limiting daily activity
- Only 1–3% per year progress to Critical Limb Ischemia (rest pain, tissue loss)
- However, the cardiovascular risk is the bigger concern: claudication patients have 5-year cardiovascular event rates (heart attack, stroke, cardiovascular death) of approximately 20–30%
This means the most important treatment goal for claudication patients isn't necessarily preventing limb loss — it's preventing heart attack and stroke through aggressive cardiovascular risk factor management.
Treatment for Intermittent Claudication
1. Supervised Exercise Therapy (First-Line)
The 2024 ACC/AHA guidelines give this a Class I recommendation. Walking to near-maximum claudication pain, resting, and repeating — 3 times weekly for 12 weeks — produces improvements in pain-free walking distance of 180–200% on average. Medicare covers 36 sessions. Read the complete exercise therapy guide →
2. Risk Factor Modification
Statins, blood pressure control, diabetes management, and smoking cessation are mandatory for all claudication patients — primarily to reduce cardiovascular event risk. Read about all PAD risk factors →
3. Cilostazol (Pletal)
The only FDA-approved medication for claudication symptoms. Improves maximum walking distance by 25–50% compared to placebo. Taken twice daily. Contraindicated in heart failure. Usually tried as second-line after exercise therapy or as an adjunct.
4. Endovascular Procedures
For patients with severe claudication that hasn't improved with exercise and medication, angioplasty (with or without stenting or drug-coated balloons) can dramatically improve walking distance. Success rates and durability depend heavily on the location and extent of disease. Read the full treatment guide →
5. Surgical Bypass
Reserved for complex cases not amenable to endovascular treatment. Aortobifemoral bypass for aortoiliac disease has excellent long-term outcomes (10-year patency >80%). Femoral-popliteal bypass with vein graft is preferred for femoral disease.