The ABI Score Scale at a Glance
Before we dive into each range, here's the complete reference table used by vascular specialists, based on the 2024 ACC/AHA Guidelines for the Management of Patients with Lower Extremity Peripheral Artery Disease:
| ABI Score | Classification | Interpretation | Cardiovascular Risk |
|---|---|---|---|
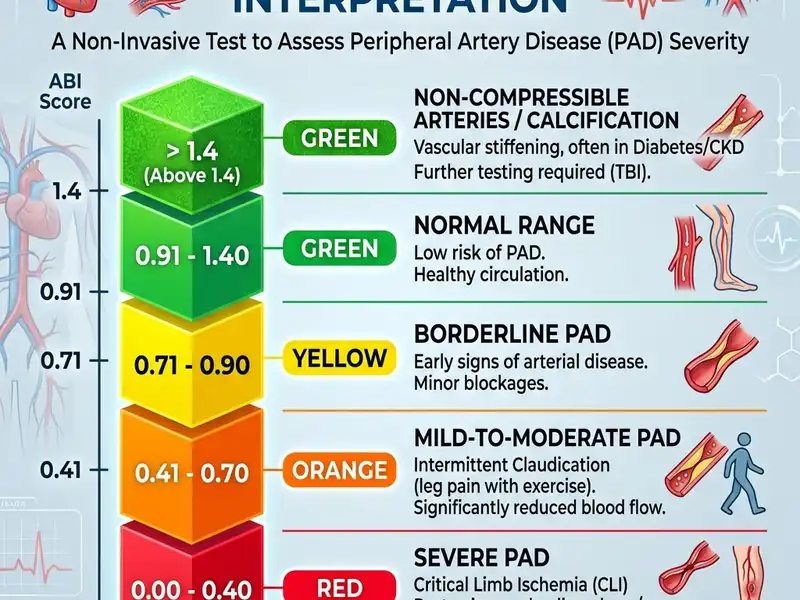
| > 1.40 | Non-Compressible | Calcified arteries; result unreliable | High — TBI test recommended |
| 1.00 – 1.40 | Normal | No significant arterial blockage | Baseline population risk |
| 0.91 – 0.99 | Borderline | Possible very early PAD | Mildly elevated |
| 0.70 – 0.90 | Mild PAD | Definite PAD; usually claudication | Moderately elevated (2× normal) |
| 0.41 – 0.69 | Moderate PAD | Significant blockage | Substantially elevated (3–4×) |
| ≤ 0.40 | Severe PAD | Critical limb ischemia risk | Very high; urgent evaluation needed |
Now let's look at each range in detail, with the clinical context that makes each one meaningful.
Normal ABI Score: 1.0 to 1.4
A score in this range — between 1.0 and 1.40 — is what we're aiming for. It means your ankle pressure is equal to or slightly higher than your arm pressure, which is the physiological norm for healthy leg arteries. Think of it as the arteries doing their job properly: wide open, flexible, and delivering blood efficiently all the way from the heart to the feet.
The "sweet spot" within the normal range is roughly 1.10 to 1.25. Scores at the lower end of normal (1.00 to 1.09) are technically normal but may warrant closer monitoring in people with multiple cardiovascular risk factors, as they can trend downward over time.
If your score is normal, does that mean you're in the clear? Mostly yes — but "normal ABI" doesn't rule out all vascular problems. Some people with early PAD have resting ABI values in the normal range but will show a significant drop during an exercise ABI test. This is called exercise-induced PAD and is more common than most people realize, especially in active individuals who push through mild leg symptoms.
What to do: Maintain healthy habits — regular exercise, a heart-healthy diet, not smoking, and controlling blood pressure and cholesterol. If you're in a high-risk group (diabetes, smoking history, over 65), recheck your ABI annually.
This is the target. Blood is flowing freely to your legs. Keep up the healthy habits that got you here — or start them now if you haven't already.
High ABI: Above 1.40 — Non-Compressible Arteries
This is where things get counterintuitive. You might expect a very high ABI to be a great sign — "my ankle pressure is way higher than my arm pressure!" But in reality, an ABI above 1.40 is a red flag, not a badge of health.
An ABI over 1.40 almost always means the ankle arteries are so hardened and calcified that they can't be compressed by the blood pressure cuff. The cuff squeezes, but the stiff, calcified walls don't collapse, so the device reads an artificially high pressure. This condition — called medial arterial calcification — is particularly common in:
- People with type 1 or type 2 diabetes (present in up to 30–40% of diabetic patients with PAD)
- People with chronic kidney disease or end-stage renal disease on dialysis
- The very elderly (age 80+)
The danger here is that these patients may actually have significant PAD — but the ABI is giving a falsely reassuring number. A Toe-Brachial Index (TBI) bypasses this problem entirely, because the tiny digital arteries in the toes are much less prone to calcification. A TBI below 0.70 is considered diagnostic for PAD when the ABI is unreliable. Read our full comparison of ABI vs TBI for more detail.
What to do: If your ABI is above 1.40, do not interpret this as normal. Tell your doctor, and ask about a Toe-Brachial Index test. Also ensure your diabetes or kidney disease is being actively managed, as these conditions drive arterial calcification.
Borderline ABI: 0.91 to 0.99
The borderline zone is, in some ways, the most clinically interesting range because it represents the transition point between healthy and diseased arteries. A score here doesn't definitively diagnose PAD — but it's the body's way of saying "something early might be happening here."
Research from the PARTNERS program — a large US study that screened over 6,000 primary care patients — found that people with borderline ABI had significantly higher rates of cardiovascular events over the next several years compared to those with normal ABI, even though most of them had no leg symptoms whatsoever.
In practical terms, a borderline ABI in a 55-year-old smoker with high blood pressure is very different from a borderline ABI in a 70-year-old non-smoker with no other risk factors. Context matters enormously.
What to do: Don't panic, but don't ignore it. This is the time to have a serious conversation with your doctor about risk factor modification — stopping smoking, controlling blood pressure and cholesterol, starting or increasing regular exercise. A repeat ABI in 6–12 months is reasonable to see if it's trending in either direction.
Mild PAD: ABI 0.70 to 0.90
An ABI in this range is a definitive diagnosis of mild Peripheral Artery Disease. The arteries are clearly narrowed enough to cause a measurable pressure drop. Many people in this range experience the classic symptom of PAD: intermittent claudication — cramping, aching, or heaviness in the calf, thigh, or buttock that appears during walking and reliably goes away within a few minutes of rest.
Some people with mild PAD have no symptoms at all — this is called asymptomatic PAD, and it's surprisingly common. The absence of symptoms doesn't mean the absence of risk. People with mild PAD carry approximately twice the cardiovascular event rate of people with normal ABI.
The good news about mild PAD is that it responds well to treatment. Supervised exercise therapy — specifically, structured walking programs — is the most evidence-backed intervention and can dramatically improve both symptoms and walking distance within 12 weeks. Statin therapy and antiplatelet treatment are typically also started at this stage.
What to do: See your doctor if you haven't already — this result warrants a proper clinical evaluation. Expect to discuss supervised exercise therapy, smoking cessation (if applicable), blood pressure and cholesterol management, and possibly aspirin or clopidogrel. Read about exercise therapy for PAD →
Moderate PAD: ABI 0.41 to 0.69
Moderate PAD represents a significant arterial blockage. At this level, most people experience frequent claudication symptoms — leg pain that limits their ability to walk even short distances. Some begin to notice discomfort at rest, particularly at night when lying flat (because gravity can no longer assist blood flow).
The risk profile at this level is substantially elevated. Data from the Framingham Heart Study and other large cohorts show that people with moderate PAD have 3 to 4 times the 10-year cardiovascular event rate of people with normal ABI. This is comparable to the risk of someone who has already had a heart attack — which is why PAD at this stage is classified as a "coronary risk equivalent" in many guidelines.
Lifestyle modifications alone are usually insufficient at this stage. Most patients need a comprehensive medical regimen, and many will be evaluated for endovascular procedures (balloon angioplasty, drug-coated balloons, stenting, or atherectomy) to physically open the narrowed arteries. Read our full guide to PAD treatment options →
What to do: This result warrants prompt referral to a vascular specialist. Don't delay. Bring this result to your doctor immediately and ask for a referral to a vascular medicine or vascular surgery clinic.
Severe PAD: ABI 0.40 or Below
An ABI at or below 0.40 indicates critical limb-threatening ischemia (CLTI) — a severe lack of blood flow to the legs and feet. This is a medical urgency. People at this level typically experience:
- Rest pain — constant burning or aching in the foot that worsens when lying down and improves slightly when the legs are dangled over the edge of the bed (because gravity helps a little)
- Non-healing wounds or ulcers — minor cuts or injuries on the feet that the body cannot heal due to inadequate blood supply
- Gangrene — in the most severe cases, tissue death can occur
Without revascularization — restoring blood flow through endovascular or surgical means — the risk of limb amputation within 6–12 months is very high. Studies show that without treatment, about 40% of patients with CLTI will require a major amputation within one year.
What to do: Seek evaluation from a vascular specialist immediately. This is not a "watch and wait" situation. Effective revascularization procedures exist and can save limbs. Time is tissue.
Does Normal ABI Change with Age or Sex?
The standard reference ranges (0.9 to 1.4 for normal) are broadly applied across adult age groups and both sexes. However, there are some important nuances:
- Age: Average ABI values tend to decline slightly with age in population studies, reflecting the natural stiffening of arteries over time. A 75-year-old with an ABI of 0.95 may be in a different clinical situation than a 45-year-old with the same score. Your doctor will interpret your ABI in the context of your overall clinical picture.
- Sex: Women with PAD are more likely to have atypical symptoms — or no symptoms at all — compared to men with the same ABI. PAD in women is often underdiagnosed for this reason. If you're a woman with a low ABI and no leg pain, don't assume you're fine.
- Race: PAD prevalence varies significantly by race. Black Americans have substantially higher PAD rates than white Americans at every age group, even after adjusting for risk factors. This disparity is believed to reflect differences in cardiovascular risk factor burden, healthcare access, and possibly biological factors.
Can You Improve Your ABI Score Over Time?
Yes — this is critically important and often under-communicated to patients. The ABI is not fixed. It reflects the current state of your arterial health, which can genuinely improve with the right interventions.
Studies on supervised exercise therapy have shown average ABI improvements of 0.10 to 0.15 points after 12 weeks of structured walking programs. For a patient starting at 0.75 (mild PAD), that could push them into the borderline or even normal range — and more importantly, their symptoms and quality of life often improve dramatically even before the ABI shows a change. Learn about supervised exercise therapy →
Smoking cessation has one of the most profound effects on ABI over time. People who quit smoking show measurably improved ABI values within 1–2 years, alongside reduced cardiovascular risk across the board. Statin therapy and blood pressure control also slow the progression of atherosclerosis, helping maintain or improve your score over time.
If you've had an endovascular procedure or bypass surgery, ABI is often used to confirm technical success — a dramatic improvement in ABI score (often jumping from 0.5 to 0.9 or above) is expected immediately after a successful revascularization. Read more about PAD treatment options →