Side-by-Side Comparison: ABI vs TBI
| Feature | ABI (Ankle-Brachial Index) | TBI (Toe-Brachial Index) |
|---|---|---|
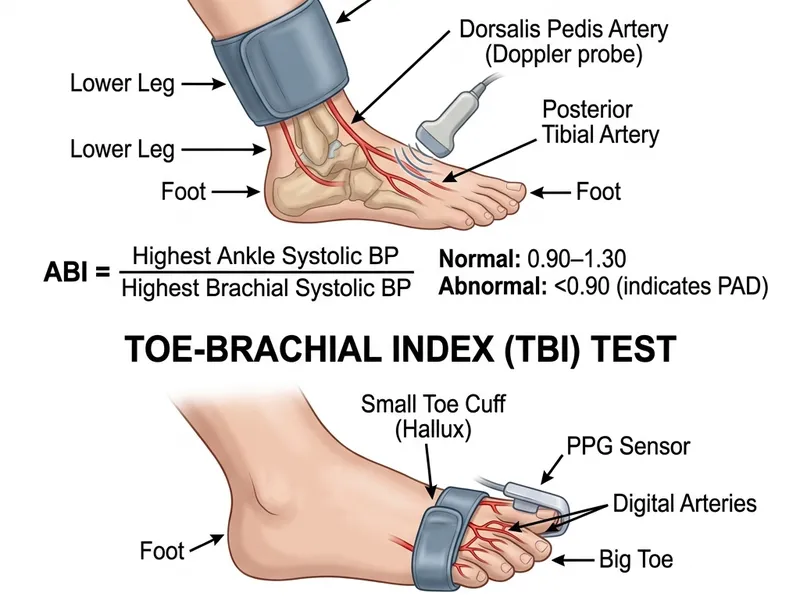
| What is measured | Ankle systolic pressure ÷ arm pressure | Toe systolic pressure ÷ arm pressure |
| Measurement site | Posterior tibial + dorsalis pedis arteries | Digital artery of the big toe |
| Detection method | Handheld Doppler ultrasound probe | Photoplethysmography (PPG) sensor |
| Normal range | 1.0 – 1.40 | ≥ 0.70 |
| PAD diagnostic threshold | ABI < 0.90 | TBI < 0.70 |
| CLTI threshold | ABI < 0.40 or ankle pressure <50 mmHg | TBI < 0.30 or toe pressure <30 mmHg |
| Affected by calcification? | Yes — falsely elevated in stiff arteries | No — toe arteries resist calcification |
| Best for | General PAD screening; non-diabetic patients | Diabetics, CKD patients, elderly, anyone with ABI >1.40 |
| Wound healing prediction | Less reliable for predicting healing | Better predictor of wound healing (toe pressure >30–55 mmHg associated with healing) |
| Availability | Widely available (most vascular labs) | Requires specialized PPG equipment — available at dedicated vascular labs |
The Core Difference: Where the Cuff Goes
The fundamental difference between the ABI and TBI tests is anatomical — specifically, where the blood pressure is measured. In the ABI, the cuff goes above the ankle. In the TBI, a much smaller cuff (sometimes called a "digit cuff") goes around the base of the big toe.
This matters enormously because of medial arterial calcification. The medium-sized arteries of the leg (tibial, peroneal, femoral) frequently calcify in patients with diabetes, kidney disease, or advanced age. This calcium stiffening prevents the cuff from compressing the artery, leading to a falsely high pressure reading.
The digital arteries of the toes — being much smaller in diameter — have comparatively little smooth muscle and rarely develop clinically significant calcification. This means the TBI remains accurate in patients where the ABI has become unreliable. Read more about how diabetes affects ABI reliability →
How Is the TBI Test Performed?
The TBI procedure is similar to the ABI but uses different equipment and a different measurement site:
- The patient lies down and rests for 5–10 minutes (same as ABI preparation)
- Arm blood pressure is measured in both arms with a standard cuff — the highest reading is recorded
- A small digit cuff (10–12mm wide) is placed around the base of the big toe on each foot
- A photoplethysmography (PPG) sensor is clipped to the tip of the big toe. Unlike the Doppler (which detects sound), the PPG sensor detects changes in light absorption caused by the pulsating blood volume — it "sees" the pulse
- The digit cuff inflates until the PPG signal disappears (flow is occluded), then slowly deflates. The pressure at which the signal returns is the toe systolic pressure
- TBI = Toe systolic pressure ÷ highest arm pressure
The test is equally painless to the ABI but requires dedicated PPG equipment. It takes slightly longer — approximately 20–30 minutes for a complete bilateral study.
Understanding TBI Results
| TBI Score | Classification | Clinical Action |
|---|---|---|
| ≥ 0.70 | Normal | No significant PAD; continue monitoring in high-risk patients |
| 0.60–0.69 | Borderline | Possible early PAD; lifestyle intervention and close follow-up |
| 0.40–0.59 | Mild-Moderate PAD | Vascular specialist referral; medical therapy optimization |
| 0.30–0.39 | Moderate-Severe PAD | Vascular specialist; evaluate for revascularization |
| < 0.30 | Severe PAD / CLTI | Urgent vascular specialist evaluation |
| Absolute toe pressure <30 mmHg | CLTI / Very low healing potential | Emergency referral — high amputation risk |
Why the TBI Threshold Is Lower Than ABI
Normal TBI is ≥0.70, while normal ABI is 1.0–1.40. Why the difference? Because toe systolic pressure is naturally lower than ankle systolic pressure even in completely healthy people, due to the progressively smaller artery diameter and higher resistance in the digital vasculature. This is normal physiology — not disease — and the TBI reference ranges are calibrated accordingly.
TBI for Wound Healing Assessment
One area where TBI is particularly superior to ABI is in predicting whether a wound on the foot will heal:
- Absolute toe pressure below 30 mmHg is associated with very poor wound healing potential and high amputation risk in CLTI
- Absolute toe pressure 30–55 mmHg — healing is possible but revascularization may be needed to improve outcomes
- Absolute toe pressure above 55 mmHg — adequate perfusion for wound healing in most patients
Wound care centers and vascular surgeons use toe pressure as a key determinant of whether a limb salvage approach (revascularization + wound care) is feasible, or whether the ischemia is too severe for the tissue to recover even with blood flow restoration.
When Should You Have a TBI Instead of (or in Addition to) an ABI?
Your doctor should order a TBI instead of (or in addition to) an ABI if:
- You have diabetes (especially long-standing or poorly controlled)
- You have chronic kidney disease or are on dialysis
- You are over age 80
- Your ABI result is above 1.40 (non-compressible arteries)
- Your symptoms strongly suggest PAD but your ABI is "normal" (ABI >0.9 but with typical claudication)
- You have a foot wound or ulcer requiring healing potential assessment
- You have known arterial calcification on X-ray or CT scan
Cost and Coverage of TBI Testing
The TBI is typically billed under CPT code 93922 (same as ABI in many settings) or 93923 for more comprehensive testing. Medicare and most private insurers cover TBI testing under the same criteria as ABI — when medically necessary for evaluation of vascular disease or wound healing assessment.
The out-of-pocket cost is similar to the ABI — typically $150–$400 in the USA for an uninsured patient. In Canada, TBI is covered by provincial health plans when ordered for medically indicated reasons, though availability varies — TBI requires specialized PPG equipment that is not as universally available as standard Doppler ABI equipment.